When treating depression, physicians often prescribe a first-line anti-depressant (e.g., Zoloft, Prozac, and Lexapro). While these treatments work for many, a significant portion find that their symptoms remain even after trying several antidepressants. Known as treatment-resistant depression (TRD), this condition affects around 30 percent of adults with major depressive disorder (MDD).
Despite its prevalence, many are unaware of treatment-resistant depression, how to determine if they might have it, or what to do about it.
Explore answers to these questions and more below.
When is Depression Treatment Resistant?
Treatment-resistant depression is generally defined as a lack of response to a few adequate trials of antidepressants. However, this leaves several questions open, including:
What counts as a lack of response?
What is an adequate trial?
How many antidepressants must a patient have tried?
It’s important to note that there are no universal answers to these questions. Instead of settling them, try answering the following questions:
Have your treatments failed to make you feel good?
Do you still not feel like your old self?
Have the side effects been difficult to manage?
Answering yes to any of these questions means you’re not getting the help you need, and it’s time to talk to your physician, who can decide the next best course of action.
Risk Factors for Treatment-Resistant Depression
Though researchers are still uncovering all traits that can increase the chances of having or developing TRD, we know several factors are associated with the condition. In particular, depression is more likely to be treatment-resistant:
If it began at an early age
The longer one has had depression
The more frequent or longer lasting one’s depressive episodes are
When there are ongoing stressors
If one has other physical or mental health conditions
What to Do About Treatment-Resistant Depression
Treatment-resistant depression is treatable. Below are steps you and your physician can take to alleviate your depressive symptoms that haven’t responded to the first few treatments.
Confirm your diagnosis: Depression that co-occurs with or is caused by other mental health conditions may require a different treatment protocol. As a result, your physician should confirm your diagnosis if your depression isn’t improving in response to treatment.
Add on talk therapy: Medications often work best when combined with some form of talk therapy. If you find your depression hasn’t responded adequately to your antidepressants, adding on therapy can give them a boost and help alleviate symptoms.
Change your medications: Just because a few medicines haven’t worked doesn’t mean none will. Newer anti-depressants (e.g., Spravato and Auvelity) that act on different neurotransmitters than first-line treatments can provide relief even when the standard solutions haven’t worked.
Try a non-medication-based intervention: While oral antidepressants are the most common medical treatment for depression, other options exist. For example, transcranial magnetic stimulation (TMS) is a non-invasive procedure where magnetic pulses are used to modulate activity in parts of the brain associated with mood regulation and is FDA approved for treatment-resistant depression.
How We Treat TRD at Heading Health
At Heading, we offer a comprehensive set of solutions to tackle TRD from every angle and provide rapid and sustained relief. We work hard to ensure that cost is not a barrier to accessing the interventions you need. We work with most insurance plans, from United Healthcare to Medicare to Blue Cross Blue Shield, and can provide coverage for all of our services, including ketamine, Spravato, and TMS, for most patients with TRD. Click here for a complete list of participating providers and to schedule a consultation to see whether our solutions are right for you.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
Over the past few years, psychedelics such as LSD and psilocybin mushrooms have garnered much attention as researchers explore their potential use in treating mental health conditions.
Ketamine and its close cousin Spravato (esketamine) are often included in this motley crew of psychedelics due in part to their “mind-altering” effects.
Though many are eager to label ketamine a psychedelic, others are less certain, feeling it would be most appropriate to avoid associating ketamine with psychedelics. Let’s explore these different viewpoints to get a clearer sense of whether ketamine is genuinely a psychedelic and why the label matters if it does at all.
What is a Psychedelic?
One obvious way of determining whether ketamine is a psychedelic is by comparing its features to those listed in its definition. Unfortunately, there are no agreed-upon criteria for what makes something a psychedelic drug. Experts waver on the importance of three conditions.
#1: Psychedelics Cause Altered States of Consciousness
Though there is much disagreement about what counts as a psychedelic, it’s generally accepted that they must induce specific mind-altering effects. Some argue this is all that is required. In other words, they claim that as long as the substance causes a “psychedelic experience,” then it’s a psychedelic.
But what are psychedelic experiences? While the list is potentially endless, psychedelic experiences are generally thought to impact one’s perception of themselves and the world around them, alter the way they think and reason, and provide insights into how their mind works and the nature of reality. They include experiences like the sense of being at one with the world, distortions of space and time, profound inner peace, ego dissolution, and many more.
#2: Their Conscious Effects Must Have Therapeutic Benefits
While many agree that psychedelics must cause certain altered states of consciousness, some argue that this isn’t enough. They claim that these changes in thought and perception must have a therapeutic effect on the mind or promote psychological growth. As Dr. Yehuda, director of the Center for Psychedelic Psychotherapy and Trauma Research at Mount Sinai Hospital in New York, notes when discussing ketamine’s status as a psychedelic:
The unanswered question in all of this is whether the transpersonal state is what heals you or whether it’s something about the molecule. […] The dissociation or psychoactive effects of ketamine might be incidental. They occur. But that’s not necessarily why the healing is happening.
For these experts, if ketamine’s mind-altering effects have nothing to do with its mental health benefits, then it’s not a psychedelic.
#3: Psychedelics Must Act on Specific Areas in the Brain
In the world of psychedelics, some have been around for longer than others and are more well-studied. For example, mescaline and psilocybin mushrooms have been used since ancient times and were researched heavily in the 1950s and ‘60s. These compounds all appear to affect serotonin (a chemical messenger in the brain) at the “2A” receptor.
Some researchers feel these “classical psychedelics” are the only true ones and that what really matters when deciding whether to categorize a new agent as a psychedelic is how it works in the brain. As Dr. Yehuda notes:
When we talk about chemistry and drug development, we should mostly be defining a psychedelic drug on the basis of the chemistry of the molecule, its pharmacokinetics, and its mechanism of action.
Does Ketamine Meet These Conditions?
How does ketamine stack up against these criteria? As far as its effects on the brain go, ketamine does not act as the classical psychedelics do. It works on N-methyl-D-aspartate (NMDA) receptors, causing an increase of glutamate and brain-derived neurotrophic factor (BDNF) instead of serotonin. Under this condition, then, ketamine is not a psychedelic.
Credit: Yang H. Ku/C&EN
However, acting on a specific set of serotonin receptors is not the only way to produce psychedelic experiences. As Dr. Steve Levine, co-founder of Heading Health, states:
It does appear that subjective psychedelic effects may be induced by a number of stimuli or conditions that also include sensory deprivation, virtual reality, meditation, and suggestibility, among others, and not necessarily mediated through a particular brain receptor.
Importantly, many of these psychedelic experiences can be produced by ketamine. It is most commonly associated with dissociative experiences (i.e., the sense that one is separate from their thoughts and body). It can also cause distortions in one’s perception of space and time. Patients have also reported gaining new perspectives and an enhanced ability to make sense of their thoughts. Rarely, ketamine can cause delusions and delirium, otherwise known as psychotomimetic effects. In many ways, then, ketamine seems to have the right sorts of effects on the mind to be considered a psychedelic.
However, it’s worth highlighting that the experiences won’t be identical to “classical psychedelics.” For example, psilocybin appears more likely to cause what’s known as ego dissolution, where one loses their subjective sense of self. Classical psychedelics may also have a greater tendency to induce visual distortions. In general, because they have different effects on the brain, their conscious effects will differ. As Dr. Arif Noorbaksh, Psychiatrist at Heading, states:
Ketamine is distinct because it works on a completely different neurotransmitter system (glutamate), exerts an effect in different areas of the brain, and as a result, the perceived effects are different. They both result in non-ordinary states of consciousness, but the experience a particular person has when exposed to conventional psychedelics versus ketamine will be different.
When it comes to the therapeutic effects of the altered states of mind that ketamine puts subjects in, the evidence is mixed. A 2020 review concluded that overall, the evidence does not suggest that ketamine’s dissociative effects are responsible for its antidepressant properties. Others argue that ketamine’s ability to cause a shift in perspective and increase cognitive flexibility and open-mindedness are directly responsible for its therapeutic effects. For example, Celia Morgan, professor of psychopharmacology at theUniversity of Exeter, found in a recent experiment that individuals who underwent ketamine and talk therapy experienced longer-lasting antidepressant effects. Professor Morgan notes that talk therapy “requires that individuals think differently about things and learn new ways of thinking about old problems.” As a result, ketamine’s ability to induce shifts in perspective and open-mindedness may explain why it appears to enhance the effects of therapy alone.
Where does this leave us? According to some criteria, ketamine seems to be a psychedelic, while on others, it does not. The answer as to whether ketamine is a psychedelic, then, depends on who you ask and which criteria they feel are most essential.
Does it Matter What We Call It?
Some might think this is all just semantics and that there’s no real principle we can use to determine what to call ketamine.
While the dispute may be verbal, how we talk about ketamine matters. As Dr. Noorbaksh notes:
I think it matters insofar as the term “psychedelic” comes with preconceived notions for many people, and it also places the emphasis on the acute effects of the agent rather than the potentially longer-term effects these agents can have on neuroplasticity, relation to self and others, and other important contributors to mental health.
As a result, it’s important to be mindful of the language we use to describe and categorize ketamine and to avoid clinging to one label or another without regard for how this impacts patients. As Dr. Levine suggests:
Ultimately, whether a molecule is “truly” a psychedelic is likely beside the point. […] Let’s not let feeling precious about terminology distract from the real goal, which is improving well-being in a safe and responsible way.
Talk with your doctor to determine whether this treatment is right for you, or you can schedule an appointment with someone from our team of psychiatrists or therapists to advise you on this or any other potential treatments for depression, including ketamine, Spravato, and TMS. Call us at 805-204-2502 or request an appointment here.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
Ketamine Vs. Esketamine (Spravato) - What’s the Difference?
October 18, 2022
Source: NeuroMend
In 2019, 19 years after researchers first demonstrated ketamine’s therapeutic effects on depression, the Food and Drug Administration (FDA) approved Janssen Pharmaceuticals’ esketamine nasal spray(Spravato) for treatment-resistant depression. In 2020, it was also approved by the FDA for major depressive disorder (MDD) with co-occurring suicidal ideation. With similar names, ingredients, and research-backed mental health benefits, many are likely to wonder whether there are any important differences between the two and if there are any reasons for preferring one over the other.
Let’s explore how they compare.
What are They Made Of?
Ketamine, or more specifically racemic ketamine, is made up of two enantiomers (i.e. pairs of molecules that are mirror images of each other), known as r- and s- ketamine (arketamine and esketamine). Esketamine contains only the S enantiomer.
How Do They Work?
Both ketamine and esketamine are thought to work by blocking N-methyl-D-aspartate (NMDA) receptors, which causes a release of glutamate (a chemical messenger in the brain) and, ultimately, brain-derived neurotrophic factor (BDNF), which helps neurons regrow and form new connections.
Though they share this mechanism of action, esketamine has a four-fold higher affinity for the NMDA receptor, which means it is more potent.
Which is More Effective?
For some drugs, one enantiomer is more “effective” than the other, which raises the question, are ketamine and esketamine equally beneficial?
In the past few years, several randomized controlled trials have directly compared the antidepressant effects of ketamine and esketamine. However, synthesizing their findings can be difficult as the studies utilize different methods of administration, treatment durations, depression-related outcomes, and more.
Despite these obstacles, a team of researchers set out to comb through the data. They analyzed 36 randomized controlled trials comparing the efficacy of ketamine and esketamine on depression in a 2022 meta-analysis. They found that while the racemic mixture was more effective overall, the evidence suggests this is not the case when the same method of administration is used alongside doses that account for differences in potency. For example, one study found that when administered intravenously and in equally potent doses, both formulations had similar remission rates after 24 hours.
Do They Feel the Same?
Both ketamine and esketamine are psychoactive substances, meaning they can alter one’s normal state of consciousness, affecting one’s thoughts, feelings, and perceptions. For example, ketamine is known for causing feelings of relaxation, dissociation, alterations in the perception of space and time, and more. A natural question, then, is whether the esketamine experience differs from the ketamine one.
Answering this question exhaustively and definitively is challenging for several reasons. To start, ketamine and esketamine can cause a wide range of experiences, so much research needs to be done to demonstrate how likely each drug is to produce each one. Second, because esketamine is more potent, it’s not always clear that researchers have used equivalent doses.
By and large, the experiences appear to be pretty similar. With that said, a few interesting preliminary findings reveal how they might differ. For example, some studies have found that ketamine is more likely to cause feelings of dissociation (i.e, a feeling of being disconnected or separate from one’s thoughts and body).
Another important result has to do with how pleasurable the experiences are. Some studies indicate that the combination of ar- and esketamine is less likely to produce unpleasant reactions like stress and anxiety. For example, one researcher found that:
The (R)-enantiomer was able to balance the (S)-enantiomer’s adverse parts of the altered state of consciousness and promote positive psychedelic experiences so that a more coherent state of consciousness is experienced.
It’s important to note that much future research will need to confirm these results and compare the drugs across all their potential subjective effects. It’s also worth pointing out that the therapeutic significance of ketamine and esketamine’s psychoactive effects is currently unclear, so any differences in how they feel may not impact how well they work.
What is the Treatment Like?
Treatments differ by how the drug is administered, the number of sessions needed, and appointment length.
Esketamine is only available as a nasal spray called Spravato. For this treatment, patients visit their physician’s office twice a week for the first four weeks, once a week for the next four weeks, and then bi-weekly if needed for maintenance. Each appointment lasts two and a half hours.
Ketamine is available in several different forms, each with a slightly different protocol. At Heading, we offer intramuscular ketamine. This treatment takes place over three weeks, with three sessions in the first week, two in the second, and one in the third. Patients may continue to receive additional treatments for maintenance if needed. Each appointment lasts around an hour and a half.
Does Insurance Cover Them?
Several insurance companies cover Spravato for treatment-resistant depression and MDD with suicidal ideation. While ketamine can be more difficult to find coverage for, our team has worked closely with insurance companies to ensure we can secure coverage for most patients. Click here for a complete list of participating providers.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
The Surprising Connections Between Caffeine and Mental Health
October 13, 2022
Between coffee, tea, soft drinks, and energy drinks, caffeine is one of the most commonly consumed psychoactive drugs. According to the Centers for Disease Control and Prevention (CDC), around 80 percent of U.S. adults consume caffeine daily.
Despite its widespread popularity or perhaps because of it, caffeine often goes under the radar as something with no significant effects other than a short boost in attention and alertness. However, caffeine can have important effects on one’s mood and overall mental health that are worth considering when deciding whether to include it in your diet.
Depression
It’s well known that caffeine can provide a short-term elevation in one’s mood. However, it may also have a beneficial effect on depression. A recent meta-analysis of seven studies found that the risk of depression decreased by eight percent per cup of coffee when consumed in moderate amounts.
The data only shows that caffeine use is correlated with lower rates of depression, not that it causes it. However, we know that caffeine promotes the release of dopamine and that dopamine deficiencies may contribute to depression. This is why some antidepressants, such as bupropion and phenelzine, modulate dopamine signaling. Additionally, when consumed from natural sources like coffee, caffeine also comes with other ingredients which can reduce inflammation and oxidative stress in the brain (more on this below).
Anxiety
Caffeine stimulates the release of cortisol, epinephrine, and norepinephrine, which are associated with feelings of stress and anxiety. This is likely why some feel anxious and jittery after a cup of coffee. Some individuals may even experience anxiety that is severe enough to warrant the diagnosis of a caffeine-induced anxiety disorder, according to the current edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-V).
Several factors may explain why some are more prone to experience anxiety from caffeine. One obvious factor is how anxious they are in general. Studies have found that patients with panic disorder, generalized anxiety disorder, and social anxiety disorder tend to experience stronger anxiety-promoting effects from caffeine.
The source of one’s anxious tendencies may play an important role in determining whether coffee makes them feel more or less nervous. For example, individuals with attention deficit hyperactivity disorder (ADHD) sometimes experience anxiety that stems from difficulties in concentration and executive control. Because caffeine can enhance attention and concentration, it can alleviate stress in individuals with ADHD.
Aside from baseline anxiety symptoms, there may also be a genetic component that explains why some individuals are more likely to experience anxiety from caffeine. Studies have found that specific gene variants for the receptor that caffeine binds to can make one more susceptible to its anxiety-inducing effects.
Interactions With Antidepressants
Caffeine can alter how our bodies process and respond to certain drugs, including some antidepressants. One way it can do this is by slowing down or speeding up the rate at which our livers break down antidepressants, impacting how much of the drugs build up in our systems.
Some antidepressants can have an activating or energizing effect. When combined with caffeine, some patients might find that the compounds work together to produce feelings of tension and anxiety. Patients should be mindful of how their body reacts to caffeine while on antidepressants and discuss any adverse reactions with their physician.
Sleep
Caffeine looks similar to a neurotransmitter called adenosine, which is partially responsible for regulating our sleep-wake cycles. When adenosine binds to its receptor, it tells the brain it’s time to sleep. Because of its resemblance to adenosine, caffeine can bind to the same receptor and block adenosine in the process. This prevents adenosine from triggering sleepiness.
Caffeine can interfere with sleep for much longer than one might initially think. This is because several of caffeine’s metabolites (i.e., the chemicals produced as the body breaks down caffeine) can also cause wakefulness. While individual factors affect how long this process takes, caffeine and its metabolites can negatively impact sleep for up to 12 hours.
A poor night’s sleep can lower one’s mood and exacerbate a range of symptoms associated with mental health conditions, so it’s important to be mindful of how caffeine affects your ability to sleep and to avoid consuming it within 12 hours of your bedtime.
Naturally Occurring Sources of Caffeine Are Better
It’s best to get caffeine from natural sources like coffee and tea instead of synthetic sources like caffeine pills or energy drinks. The reason is that natural sources of caffeine come with other healthy ingredients. For example, tea contains antioxidants that can decrease oxidative stress in the brain, a change associated with improvements in depression. Similarly, caffeine contains chlorogenic acid, an antioxidant and anti-inflammatory. Naturally occurring sources of caffeine may also include a class of compounds known as phenols, which studies have found can work synergistically with caffeine to heal our bodies and minds.
If you feel you need to see a mental health professional or could use help deciding which service is right for you, please give us a call at 805-204-2502 or fill out an appointment request here. We have a wide variety of providers, including therapists, psychiatrists, nurse practitioners, and nutritional therapists, who can see you in as little as one day via teletherapy.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
Obsessive-compulsive disorder (OCD) is a condition characterized by recurrent, unpleasant intrusive thoughts and repetitive behaviors aimed at reducing anxiety or preventing some undesirable event. It currently afflicts between two to three million U.S. adults.
The condition is typically treated with some combination of cognitive-behavioral therapy (CBT) and a type of oral antidepressant called selective serotonin reuptake inhibitors. However, studies indicate that around half of OCD patients fail to respond adequately to the standard treatments. Moreover, many that respond to SSRIs discontinue due to undesirable side effects (e.g., weight gain, sexual dysfunction, emotional numbness, etc.).
Because of this, researchers began to search for novel treatments. Many focused on finding new applications for a non-invasive procedure called transcranial magnetic stimulation (TMS), initially approved by the FDA for treatment-resistant depression in 2008. In 2018, TMS became FDA-approved for OCD.
Here are answers to common questions about this new intervention.
What is TMS?
TMS is a drug-free and noninvasive procedure used to treat various brain disorders, including several mental health conditions. It uses magnetic coils placed just above the scalp to send magnetic pulses into specific regions of the brain associated with symptoms of the conditions it is being used to treat. For example, in the case of treatment-resistant depression, the pulses are sent toward regions of the brain associated with mood regulation.
By sending repeated pulses to these specific areas of the brain, TMS “trains” neurons in those areas to fire differently and create new, healthier connections.
How Does TMS for OCD Work?
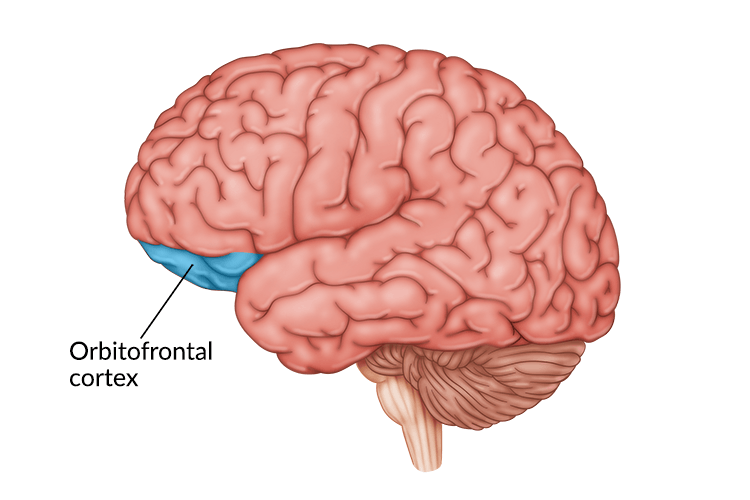
TMS for OCD works in much the same way as TMS for treat-resistant depression, except for two key differences. First, the magnetic pulses are directed at deeper structures in the brain, which are more closely associated with OCD. For example, one of the primary targets is the right orbitofrontal cortex, which studies have found is hyperactive in adults with OCD. It is also thought to be partially responsible for the unending urge to repeat compulsive behaviors that individuals with OCD experience. Other targeted areas include the supplementary motor cortex, medial prefrontal cortex, and anterior cingulate cortex.
Unlike treatment-resistant depression, which is associated with underactive neurons in parts of the brain related to mood regulation, OCD is connected with brain regions firing too much. As a result, in addition to targeting different areas of the brain, technicians utilize another type of stimulation called low wave stimulation, which inhibits, rather than activates, regional brain activity.
What are the Advantages of TMS for OCD
TMS has several advantages compared to the first-line oral medications used to treat OCD.
One of the problems with oral medications is that they are often imprecise, spreading throughout the brain and targeting many more areas than are directly implicated in the conditions they are meant to treat. This causes many unwanted side effects, such as weight gain, sexual dysfunction, emotional numbing, and more. TMS can deliver incredibly localized treatments, targeting the very source of the symptoms and avoiding unwanted side effects.
Aside from lacking precision, first-line oral medications often must be taken continuously to cause and maintain their therapeutic effects. After a round of TMS treatments, the benefits can last for a substantial period of time. On average, results last between four to fourteen weeks and can easily be sustained with quick maintenance sessions.
How Heading Does TMS for OCD Differently
In many cases, TMS is offered as a standalone treatment. While it can be very effective on its own, studies have found its effects can be amplified when combined with other interventions. For example, one experiment found that patients who underwent TMS and CBT experienced nearly a 60 percent drop in their OCD symptoms and that for 80 percent of the subjects, their symptoms decreased by at least 40 percent.
At Heading, patients have access to our integrated team of mental health specialists with wide-ranging expertise to complement their TMS and enhance its therapeutic effects. By combing TMS with other therapies, our patients benefit from the synergistic effects of a holistic approach to mental health.
Talk with your doctor to determine whether this treatment is right for you or schedule an appointment with one of our psychiatrists or therapists to advise you on this or any other potential treatments, including ketamine, Spravato, and TMS. Call us at 805-204-2502 or request an appointment here.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
The Problem of Delayed Treatment for Mental Health Conditions
October 9, 2022
From recognizing one needs treatment to finding an in-network provider to scheduling an appointment, getting help for one’s mental health can be a time-consuming and disheartening process. One study found that since 2000, individuals with schizophrenia, mood, and anxiety disorders have taken nearly 32 months on average to receive their first treatment.
Aside from the immediate harm of suffering from the symptoms of a mental illness, a delay in treatment is associated with a range of negative outcomes, highlighting the importance of prompt access to rapidly effective interventions.
Here are some key findings:
Rates of Treatment Response and Remission
When examining the impact of the duration of untreated illness (DUI) on mental health outcomes, much research has focused on rates of response (i.e., at least a 50 percent reduction in symptoms) and remission (i.e., a full recovery). A meta-analysis, which compiled data from several studies on the topic found some striking results. In particular, they found that:
Patients with a DUI shorter than eight weeks after their first episode of depression have a 70 percent greater probability of achieving a response
Patients with a DUI shorter than eight weeks after their first episode of depression have a 65 percent greater probability of achieving remission
Response to Antidepressants
Researchers looked specifically at the response to antidepressants and found similar results. For example, studies have found that:
Patients with obsessive-compulsive disorder who did not receive treatment within the first 24 months were 28 percent less likely to respond to SSRIs (selective-serotonin-reuptake inhibitors)
Subjects with major depressive disorder who did not receive a first-line antidepressant until six months or more after their depression started were 13 percent less likely to experience remission
Longer DUI was associated with a lower response to antipsychotics and a higher rate of relapse in individuals with schizophrenia
Suicide
Mental illness can bring about feelings of hopelessness and despair which can cause patients to think about or attempt to commit suicide. Several studies have found that a longer DUI is associated with more suicidal thoughts and attempts for a range of conditions. For example, studies have found that:
Bipolar patients with a longer DUI showed a higher number of suicide attempts during a five-year follow-up
In patients with schizophrenia, suicidal plans or attempts were significantly higher in subjects from communities without an early detection program relative to those from early detection communities
Depressed patients with a longer DUI also showed an increase in the number of hospitalizations and suicide attempts
Cognitive Performance
Deficits in cognitive performance (e.g., in tasks involving memory, attention, verbal abilities, etc.) have become one of the core features of mood disorders and are significantly associated with DUI. A 2020 study found that:
Over half of the subjects diagnosed with major depressive or bipolar disorder showed mild cognitive impairment.
Those with major depressive disorder who showed cognitive impairment had a six month longer DUI on average
Remission was associated with improvements in memory, executive function, and attention, but not in visuospatial abilities or verbal fluency
Physiological Changes in the Brain
Researchers have found that as mental health conditions go untreated, they can produce a range of physiological changes in the brain. For example, one meta-analysis found that:
Long durations of untreated illness are associated with brain changes in individuals who have schizophrenia, bipolar disorder, major depressive disorder, panic disorder, and obsessive-compulsive disorder
In schizophrenia, significant changes can occur within the first year
Some brain changes may be associated with poor treatment response
Associations with other Chronic Conditions
Mental illness is associated with various other chronic health conditions, such as heart disease and diabetes. Again, a longer DUI is associated with worse outcomes regarding many of these conditions. A 2022 study found that:
Subjects with depressive and bipolar disorders with DUIs longer than one and two years, respectively, were nearly 30 percent more likely to have physical comorbidities
Longer DUIs were significantly associated with higher BMIs, which can cause or exacerbate other physical conditions
Takeaways
These findings highlight two general takeaways. First, there is an obvious need to shorten the time it takes for patients to receive treatment. Given the wide range of adverse outcomes that become more prevalent as DUI increases across several mental health conditions, individuals dealing with mental illness must receive treatment as soon as possible.
Second, there is a need for novel treatments. Even when patients can see a physician, first-line treatments can take several weeks to months to work. For a sizable subset of these individuals, these solutions may not be effective, even when their illness is recent. Additionally, longer DUIs are associated with physiological changes in the brain, which may be why standard treatments tend to be less effective over time. As a result, solutions working in different ways targeting different parts of the brain, like ketamine, TMS, or other emerging interventions, may prove critical for treating individuals who do not respond to first-line treatments.
At Heading Health, we utilize a multi-pronged approach to combat these issues. First, we offer an integrated team of specialists who work together to provide prompt care tailored to each patient’s individual needs. In most cases, we can see patients within 24-48 hours. To support this approach, we use cutting-edge treatments with rapid and sustained responses, meaning patients get in and get better quickly.
Talk with your doctor to determine whether these treatments are right for you, or schedule an appointment with one of our psychiatrists or therapists to advise you on any other potential treatments for depression, including ketamine, Spravato, and TMS. Call us at 805-204-2502 or request an appointment here.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
Interview with an Expert: Should Ketamine Be Combined with Psychotherapy?
October 7, 2022
With evidence mounting in support of ketamine’s therapeutic effect on depression and other mental health conditions, clinics and physicians are increasingly prescribing it as a standalone solution. While ketamine has clear benefits on its own, experts are beginning to explore the role psychotherapy plays in enhancing or extending its effects.
In a recent edition of The Peter Attia Drive, Professor of Psychopharmacology and leading ketamine scholar Celia Morgan addresses this topic, among several others related to ketamine’s use in treating depression and other mental health conditions.
Her take? Psychotherapy is critical to obtaining a lasting effect from ketamine. Here’s why.
Ketamine Increases Neural Plasticity
One of the key reasons Professor Morgan believes ketamine is most effective when combined with psychotherapy is its mechanism of action (i.e., how it changes the brain to produce its therapeutic effects).
When ketamine enters the brain, it attaches to N-methyl-D-aspartate (NMDA) receptors, causing a release of glutamate (a chemical messenger in the brain) and brain-derived neurotrophic factor (BDNF). The result is that neurons (tiny cells in the brain that send and receive information from each other) have an increased ability to grow, reorganize, and rewire themselves in response to new experiences, a phenomenon known as neural plasticity.
Among other things, neural plasticity enables us to learn and acquire new habits, including our cognitive and emotional tendencies. Professor Morgan argues that because many psychological therapies target these mental habits, they may be more effective when used after ketamine treatments. She states:
We know that what we’re asking people to do in psychological therapy is to think differently about things and learn new ways of thinking about old problems. [Neural plasticity] seems to me like an intuitively appealing mechanism.
Professor Morgan goes on to suggest that not only might therapy be beneficial but that its precise timing after a ketamine treatment may be especially critical, stating:
I think the idea you know for me as a psychologist is that you could time your psychological therapy when your brain is most plastic. […] We know from animal studies this might be starting four hours following the ketamine days peaking about 24 hours.
Ultimately, more research needs to be done to determine when ketamine causes the greatest increase in neural plasticity in humans. Professor Morgan notes that:
We want to be doing some work at the moment to sort of chart the time course of that in humans by looking at EEGs […] and trying to target the window of this synaptic plasticity
Experimental Participants Receiving Therapy Maintain Therapeutic Benefits for Longer
Ketamine’s impact on neural plasticity suggests that ketamine should enhance the effects of psychotherapy in theory, but how does this pan out in practice?
In a recent study on the effectiveness of ketamine in the treatment of alcohol use disorder, Professor Morgan compared the effects of ketamine used on its own and when combined with psychotherapy. They found the greatest reductions in drinking and abstinence in the group that received ketamine alongside psychological therapy.
What’s particularly shocking is that 86 percent of the ketamine therapy subjects remained abstinent for six months after three ketamine infusions. Given the small number of treatments, the six-month benefit patients experienced further suggests therapy had a positive impact. As professor Morgan highlights, studies show the antidepressant effects of a single IV ketamine infusion typically last from three days to a week, though repeated administrations can extend this effect.
Conclusion
While more research is needed to confirm and clarify therapy’s role in enhancing and extending the effects of ketamine on depression and other mental health conditions, these early results suggest the two therapeutic solutions work synergistically to deliver an optimal outcome.
Talk with your doctor to determine whether this treatment is right for you or schedule an appointment with one of our psychiatrists or therapists to advise you on this or any other potential treatments for depression, including ketamine, Spravato, and TMS. Call us at 805-204-2502 or request an appointment here.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
Transcranial magnetic stimulation (TMS) is a non-invasive, drug-free procedure that uses magnetic coils to stimulate and influence the brain’s activity. Utilizing a unique mechanism entirely different from the standard array of psychiatric medications, TMS represents an important alternative for individuals who have not responded to other treatment options.
Below are answers to some common questions about TMS.
How Does TMS Work?
Most currently available medical treatments for psychiatric conditions require patients to ingest a drug that eventually enters the brain and alters its functioning in ways that alleviate symptoms of mental illness. For example, selective serotonin reuptake inhibitors, such as Prozac, Zoloft, and Lexapro, latch on to parts of neurons (tiny nerve cells in the brain) and prevent them from reabsorbing serotonin, a change which has been linked to improvements in anxiety, depression, and other conditions.
In contrast to these treatments, TMS is drug-free and noninvasive, meaning its active ingredient is not something that must be ingested or implanted. Instead, TMS impacts the brain from the outside. More specifically, it uses magnetic coils placed just above the scalp to send magnetic pulses into specific regions of the brain associated with mood regulation.
In turn, these pulses induce a series of changes in the brain that improve mood and alleviate symptoms of depression. As Latitia McDaniel, assistant TMS program director at Heading Health states:
By targeting these specific areas of the brain, TMS stimulates and strengthens these neural pathways. Like training a muscle, over time, the inactive signals begin firing and reconnecting properly again, thus restoring the emotional control center.
What Is It Used to Treat?
TMS is approved by the U.S. Food and Drug Administration (FDA) to treat the following conditions:
In addition to being FDA-approved, treatment-resistant depression (i.e., depression that has not adequately responded to one or more antidepressant drugs) is now covered by several insurance companies. At Heading, we work with most insurance plans, from United Healthcare to Medicare to Blue Cross Blue Shield. Click here for a full list of participating providers and to schedule a consultation to determine whether TMS is covered for you.
Aside from the above-mentioned conditions, researchers continue to examine whether TMS might be useful for other mental illnesses not currently approved by the FDA, including:
Bipolar disorder
Eating disorders
Generalized anxiety disorder
Panic disorder
Schizophrenia
Substance abuse
Post-traumatic stress disorder.
What Is the Treatment Like?
TMS treatment for Major Depressive Disorder typically consists of three-minute or 20-minute sessions that occur five days a week over six weeks.
Undergoing TMS is a quick and straightforward process. At each appointment, patients sit in a relaxing chair as the practitioner places the magnetic coil in the correct location on their head. As the treatment begins, patients may feel a light tapping on their head that eventually dissipates. While rare, some individuals may feel some discomfort on their scalp, though this can be resolved by rotating or moving the magnetic coil or through other easy modifications.
After the session has ended, patients are free to drive home and continue their day as usual.
How Does Heading Health Do TMS Differently?
At Heading health, we focus on utilizing the best available tools to ensure our treatments are delivered precisely, reliably, and consistently.
One of the ways we accomplish this with TMS is with the Magstim StimGuide, the first navigational system specifically designed for the clinical market. After the target location has been identified, the StimGuide stores the location using four distinct parameters captured by a 3D snapshot of the treatment area. When administering TMS, this tool helps practitioners consistently identify the target area by emitting a green light when all four parameters are aligned.
In addition, our machines come outfitted with MagStim’s E-Z Cool Coil Coil, which has a built-in intelligence cooling system capable of at least a 37-minute protocol.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
What's Does Spravato Feel Like? A Patient's Perspective
October 3, 2022
This post was written by a member of our team currently receiving treatment, using Spravato, in Michigan where he resides. He wanted to share his story with us in hopes that it might help patients seeking care with Heading. While he is not a patient of Heading (as Heading provides care to patients in Texas) his treatment program, environment, and experiences detailed in his share are very similar to those at Heading. We are grateful he chose to share his story with us.
I have suffered from anxiety and depression for most of my life. Treatment began at age 12 when I was diagnosed with generalized anxiety and obsessive-compulsive disorder (OCD). While the initial treatments helped to some degree, many symptoms remained, and the side effects of the drugs I took became intolerable.
Over the next 17 years, I switched from one oral antidepressant to the next, desperately trying to find something that addressed my symptoms without causing side effects that were worse than what I was trying to treat. Eventually, my psychiatrist recommended a drug called Spravato (esketamine nasal spray), a rapid-acting drug used for treatment-resistant depression. He told me that Spravato works differently than traditional antidepressants by increasing levels of glutamate and brain-derived neurotrophic factor (BDNF). These two changes have been associated with improvements in depression and anxiety. Knowing this, I felt hopeful that I might get the benefits I was looking for without the drawbacks I was trying to avoid.
Though I was excited about trying out the new intervention, I grew increasingly anxious as I awaited my first treatment session. Both esketamine (the active ingredient in Spravato) and its more famous cousin, ketamine, are psychoactive, meaning they can alter one’s normal state of consciousness, affecting one’s thoughts, feelings, and perceptions.
Before trying Spravato, I had very little experience with psychoactive drugs and none with anything that might be considered a psychedelic. As a result, I had no idea what to expect. To make matters worse, I felt that I wouldn’t react well to the experiences that Spravato might bring about because I suffered from severe anxiety. I went into my appointment blind to what I was about to experience. Though my fears were unwarranted, I would have benefited greatly from a clear and honest description of what was to come.
My Experience with Spravato
Below I describe to the best of my ability what I typically feel during a Spravato treatment session. Though some of these experiences may generalize, it’s important to remember that everyone’s brain is unique and may react differently to Spravato.
Dissociation
One of the more talked about effects of Spravato is its ability to cause dissociation. Though it is described differently by different people, the effect is generally characterized as a temporary feeling of disconnection from one’s thoughts and feelings.
I like to describe my personal experiences with dissociation as akin to the sensation one gets when looking at their avatar through a virtual reality headset. Everything is in the location it’s supposed to be and moves when it should, but you don’t identify with your avatar. Its movements don’t feel like your movements. Its body doesn’t feel like your body.
The feeling of separation from my thoughts is harder to describe. The best I can say is that it feels like I am “viewing” my thoughts rather than “thinking” them. They simply pass by, unauthored by me.
Feeling of Relaxation
Despite having unusual sensations like the feeling of dissociation, I often experience a wave of relaxation as my concerns and worries drift away. My thoughts quiet down, and former troubles begin to feel like they don’t matter as much.
Feelings of Stress and Anxiety
Though Spravato can be pleasurable, it can also be unpleasant and stressful. I believe this is at least partially the result of the following two factors.
First, while under the effects of Spravato, my mind tends to focus on unpleasant thoughts at the core of many of my worries (more on this below). Though these thoughts are easier to entertain at the time, they can still be challenging to confront.
Second, aside from its psychological or psychoactive effects, Spravato causes physical sensations that tend to be more unpleasant. For example, I often get dizzy and feel like I am slowly spinning in my chair. As a result, I feel nauseous. When these sensations become too intense, the overall experience can become quite stressful. Fortunately, my doctor prescribed an antiemetic (i.e., an anti-nausea drug), so these sensations have become less frequent and more tolerable.
Increased Empathy
The state that Spravato puts me in makes it easier for me to put myself in other peoples’ shoes. Often, I will spend time thinking about past arguments or disagreements. While doing so, I have an easier time understanding where the other person was coming from and why their reactions and feelings were appropriate. More generally, I tend to have a stronger concern for the well-being of others.
Enhanced Ability to Confront Unpleasant Thoughts
Through my Spravato experiences, I have realized that at the heart of many of my daily fears are more general worries that I have trouble recognizing or confronting. While under the effects of Spravato, my attention is almost unavoidably directed toward these fundamental concerns
Here’s a personal example to shed light on how this works. Among the many things I worry about, work is often at the top of the list. I worry while working on assignments, submitting them, waiting for feedback, etc. Though I had spent so much energy feeling anxious about this, I never looked at the underlying concern or belief that connected all these more specific worries. During one Spravato treatment, I realized that I had deep concerns about my intellectual abilities and that I viewed each work assignment as a potential instance where my real lack of capability would be revealed.
Though the fear remains, knowing it exists and is responsible for so many other specific worries has made it easier to deal with.
Visual Distortions
Around 10 minutes into each treatment, I start to notice some visual effects. First, my vision becomes fuzzy, and I have trouble refocusing each time I move my eyes. Over the next few minutes, this effect increases in intensity until everything looks as though it is shaking for a few seconds after I shift from looking at one spot to another.
Aside from becoming fuzzier and shakier, my vision tends to change in a different way. Specifically, objects appear to be slowly expanding and contracting as if they are breathing. Often, I’ll try to match my breath to the rate at which the things are “breathing.” It’s pretty relaxing.
When I close my eyes, I notice a further visual effect. As I keep them shut, I see faint geometric patterns. This is especially noticeable when my eyes are almost but not completely closed, which happens to me somewhat frequently when dozing off under Spravato. My guess is that my brain is doing its best to interpret the unusual visual stimuli it is getting, and the result is that I have some minor closed-eye visuals.
Post-Treatment Effects
Though many of the effects subside by the end of the two-hour treatment, some remain for several hours. I tend to feel tired, off-balance, and a bit groggy. These effects slowly dissipate as the day goes on but do not linger into the next day.
Concluding Thoughts
From enhanced empathy to feelings of dissociation, Spravato experiences can feel intense or overwhelming when you don’t know what to expect. After I learned first-hand what the experience feels like, my Spravato sessions became much more relaxing and pleasant. Hopefully, my descriptions will help other anxious patients get there more quickly.
Stay tuned for part two of this blog, where I describe the long-term effects of Spravato on my depression and anxiety.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.
When trying to treat depression and anxiety, most people turn to psychotherapy, oral medications, or some other medical intervention.
While these treatments are effective and often a vital part of many individuals’ mental health toolkits, they aren’t the only ways to prevent and treat mental illness. In particular, research increasingly suggests that our diets can have a significant impact on our mental health. For example, a 2017 study found that around a third of subjects who switched to a Mediterranean-style diet no longer had symptoms of depression by the end of the trial, compared to eight percent of the participants who made no dietary changes.
Nutritional therapists utilize these findings to help patients with a wide range of conditions by offering evidence-based, individualized advice on dietary and other lifestyle changes they can make to support their bodies and, in turn, their minds.
Let’s look at some answers to common questions about nutritional therapy and its role in mental health.
How Does Nutritional Therapy Impact Mental Health?
It’s common knowledge that what we eat can impact our physical health. For example, it’s well known that eating a diet high in sugar can increases one’s odds of developing diabetes and that high cholesterol, high sodium diets can increase the risk of developing heart disease.
But how can nutrition have an impact on mental health conditions? While the connections between diet and mental health are complex, there are, essentially, two ways in which what we eat can improve or harm our mental well-being.
First, the nutrients in our food get sent to the brain, altering its functioning in various ways that can impact mental health. For example, antioxidants, found in high levels in fruits and vegetables, can make their way into the brain and decrease oxidative stress, which has been implicated in several mental illnesses. Second, they can impact the health of our gut microbiomes. This collection of bacteria, viruses, fungi, and microbes performs a variety of roles, from producing some of the brain’s serotonin to regulating immune function, which can impact brain health and, ultimately, our psychological well-being.
What Conditions Can Nutritional Therapy Be Used to Treat?
From depression to schizophrenia, nutritional therapy can be used to treat a wide range of mental health conditions. This is partly because many mental disorders are caused or exacerbated by a set of common factors one can impact with their diet. As our resident expert and registered dietician, Sally Twellman notes:
Inflammation appears to be a common factor in mental illness, and dysfunction in the gut is often at the root of chronic inflammation. When you look at the research, regardless of the manifestation of mental illness, symptoms typically improve by decreasing inflammation and replenishing the micronutrients that one needs to thrive. And this is really across the board.
How Does Heading Health do Nutritional Therapy Differently?
Heading Health’s approach to nutritional therapy is unique in several important ways.
First, our nutritional therapy can be combined with in-house teletherapy or telepsychiatry. This is critical because nutritional therapy is often best used to amplify the effects of other treatments, like psychotherapy or medications, rather than as a stand-alone solution. Second, we utilize a holistic, evidence-based approach, which encompasses more than the standard dietary changes, like those involving proteins, calories, and carbs. As Sally notes when discussing her approach to nutritional therapy:
Often when we discuss nutrition modification, we only focus on proteins, calories, fat, and carbohydrates. That’s important. But then we often forget that the real medicine in our food comes from vitamins, minerals, and phytochemicals. If we don’t have those basic building blocks and we don’t have those correct signaling molecules, it’s difficult for our brains to function optimally.
Importantly, we don’t stop at dietary changes. We also include lifestyle modifications (e.g., exercise, meditation, journaling, breathwork, etc.), which are known to positively affect mental health and can enhance the effects of dietary alterations.
Overall, we look at the whole person and consider how they can make small but meaningful adjustments that complement other treatments they are receiving to optimize their mental health.
Take the first step
Want to find out if Heading is right for you?
Complete our consultation form and an intake specialist will get in touch.

 When treating depression, physicians often prescribe a first-line anti-depressant (e.g., Zoloft, Prozac, and Lexapro). While these treatments work for many, a significant portion find that their symptoms remain even after trying several antidepressants. Known as treatment-resistant depression (TRD), this condition affects around 30 percent of adults with major depressive disorder (MDD).
When treating depression, physicians often prescribe a first-line anti-depressant (e.g., Zoloft, Prozac, and Lexapro). While these treatments work for many, a significant portion find that their symptoms remain even after trying several antidepressants. Known as treatment-resistant depression (TRD), this condition affects around 30 percent of adults with major depressive disorder (MDD).

 Over the past few years, psychedelics such as LSD and psilocybin mushrooms have garnered much attention as researchers explore their potential use in treating mental health conditions.
Over the past few years, psychedelics such as LSD and psilocybin mushrooms have garnered much attention as researchers explore their potential use in treating mental health conditions.  Though there is much disagreement about what counts as a psychedelic, it’s generally accepted that they must induce specific mind-altering effects. Some argue this is all that is required. In other words, they claim that as long as the substance causes a “psychedelic experience,” then it’s a psychedelic.
Though there is much disagreement about what counts as a psychedelic, it’s generally accepted that they must induce specific mind-altering effects. Some argue this is all that is required. In other words, they claim that as long as the substance causes a “psychedelic experience,” then it’s a psychedelic. 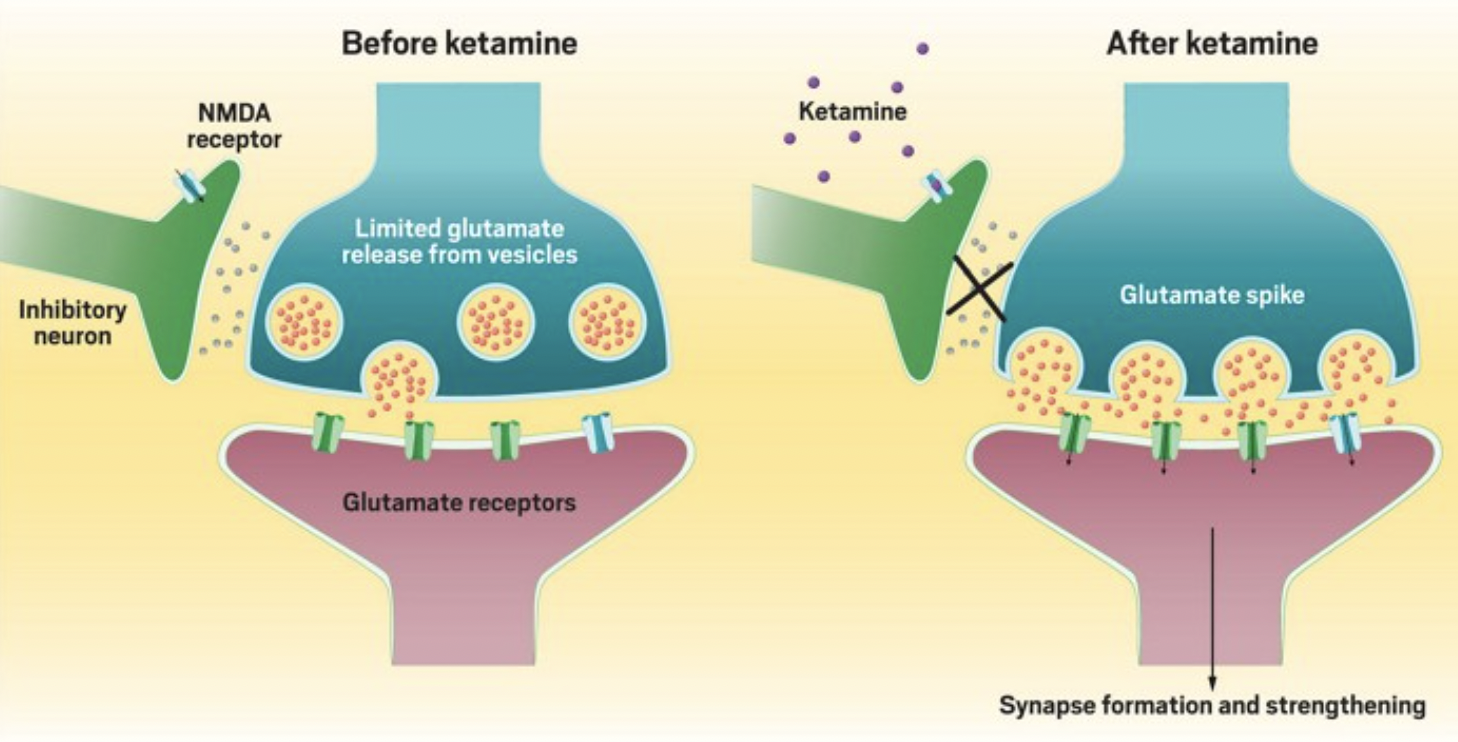


 What are They Made Of?
What are They Made Of? 


 Between coffee, tea, soft drinks, and energy drinks, caffeine is one of the most commonly consumed psychoactive drugs.
Between coffee, tea, soft drinks, and energy drinks, caffeine is one of the most commonly consumed psychoactive drugs. 




 From recognizing one needs treatment to finding an in-network provider to scheduling an appointment, getting help for one’s mental health can be a time-consuming and disheartening process. One
From recognizing one needs treatment to finding an in-network provider to scheduling an appointment, getting help for one’s mental health can be a time-consuming and disheartening process. One 



 Mental illness is associated with various other chronic health conditions, such as heart disease and diabetes. Again, a longer DUI is associated with worse outcomes regarding many of these conditions. A 2022
Mental illness is associated with various other chronic health conditions, such as heart disease and diabetes. Again, a longer DUI is associated with worse outcomes regarding many of these conditions. A 2022 

 One of the ways we accomplish this with TMS is with the Magstim StimGuide, the first navigational system specifically designed for the clinical market. After the target location has been identified, the StimGuide stores the location using four distinct parameters captured by a 3D snapshot of the treatment area. When administering TMS, this tool helps practitioners consistently identify the target area by emitting a green light when all four parameters are aligned.
One of the ways we accomplish this with TMS is with the Magstim StimGuide, the first navigational system specifically designed for the clinical market. After the target location has been identified, the StimGuide stores the location using four distinct parameters captured by a 3D snapshot of the treatment area. When administering TMS, this tool helps practitioners consistently identify the target area by emitting a green light when all four parameters are aligned.